Effective Dose of Two CBCT and Panoramic Radiography Hybrid Devices Using a DAP-Based Method
* Kirnbauer Barbara;
Rugani P;
Guss H;
Stücklschweiger G;
Jakse N;
-
* Kirnbauer Barbara: Department of Dental Medicine and Oral Health, Division of Oral Surgery and Orthodontics, Medical University of Graz, Graz, Austria.
-
Rugani P: Department of Dental Medicine and Oral Health, Division of Oral Surgery and Orthodontics, Medical University of Graz, Graz, Austria.
-
Guss H: Competence Center of Medical Physics and Radiation Protection, University Hospital Graz, Graz, Austria.
-
Stücklschweiger G: Competence Center of Medical Physics and Radiation Protection, University Hospital Graz, Graz, Austria.
-
Jakse N: Department of Dental Medicine and Oral Health, Division of Oral Surgery and Orthodontics, Medical University of Graz, Graz, Austria.
-
Oct 15, 2021 |
-
Volume: 2 |
-
Issue: 3 |
-
Views: 1368 |
-
Downloads: 853
-
Download PDF
Abstract
Objectives: With Cone-Beam Computed Tomography (CBCT) established in daily dental practice, there is an urgent need to raise awareness of the radiation risk it poses and to encourage training in its safe use. This study aimed to evaluate the effective doses of all possible field of view modes and varying recording settings of two-/ three-dimensional (2D/3D) hybrid machines.
Methods: Using an MC-based software, effective doses with the Planmeca Promax 3D Max (Planmeca OY, Finland) and the Sirona Orthophos XG 3D (Dentsplysirona, Germany) were evaluated in the 2D and 3D modes for both juvenile and adult patients.
Results: Effective doses of 3 μSv to 650 μSv for the 3D modes were recorded at both devices, while for the Panoramic Radiography (PR) model, doses were between 6 μSv to 16 μSv. Dose Area Product (DAP) calculations showed variations for PR (mean 26.2%) and CBCT (mean 3.8%) compared to DAPs specified by the manufacturer.
Conclusions: Results demonstrated a wide range of effective doses, strongly depending on the image mode chosen, as well as on individually chosen parameters such as field of view (FoV), resolution mode, and patient size. It could be confirmed that using the ULD mode substantially decreases radiation doses.
Clinical Relevance: Based on the wide range of dose results, the authors of this study underline the necessity of advanced training for personnel using X-ray devices in dentistry, especially when 3D modes are applied.
Introduction
Though dental X-ray is an indispensable diagnostic tool in routine dental practice, [1] with two-dimensional (2D) techniques such as Panoramic Radiography (PR) forming the basis of radiological diagnostics, Cone Beam Computed Tomography (CBCT) is also becoming internationally established as an in-house three-dimensional (3D) tool with reasonable costs and doses. The market is constantly growing and currently offers up to 85 different machines with a variety of possible recording settings [1] and a wide range of effective doses applied to patients [2]. Especially with the full skull mode, dosages may become comparable to those reached with Multislice Computed Tomography (MSCT), thereby calling into question the most advertised advantage of CBCT as a dose-saving cross-sectional imaging alternative [3,4]. This study aimed to evaluate the effective doses based on calculated dose area products (DAPs in mGy.cm2) of all possible field of view modes and varying recording settings of two-/ three-dimensional (2D/3D) hybrid machines.
Methods
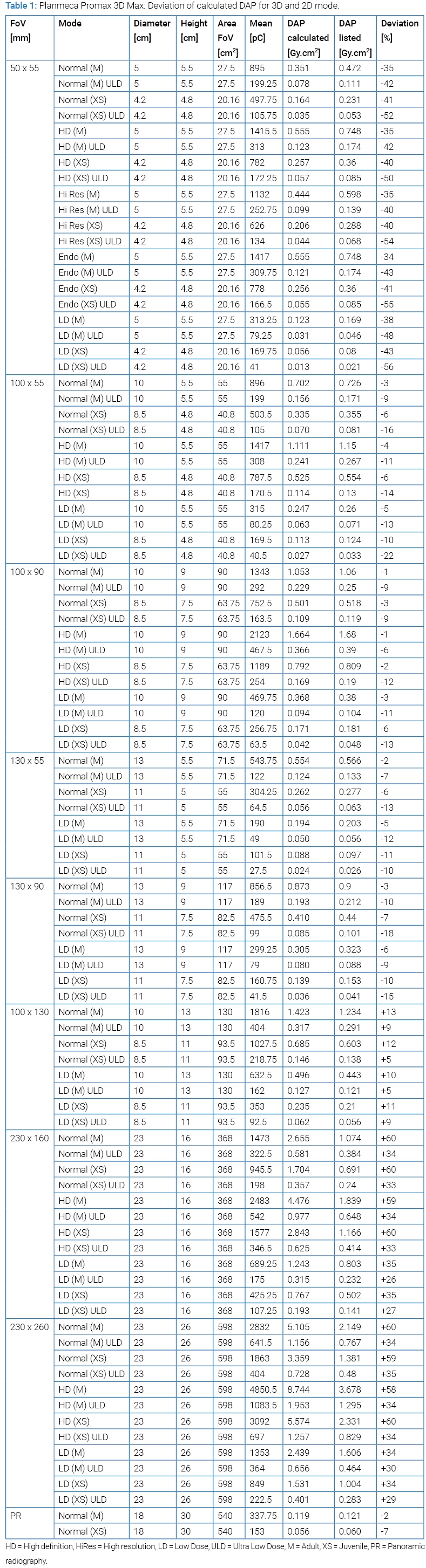
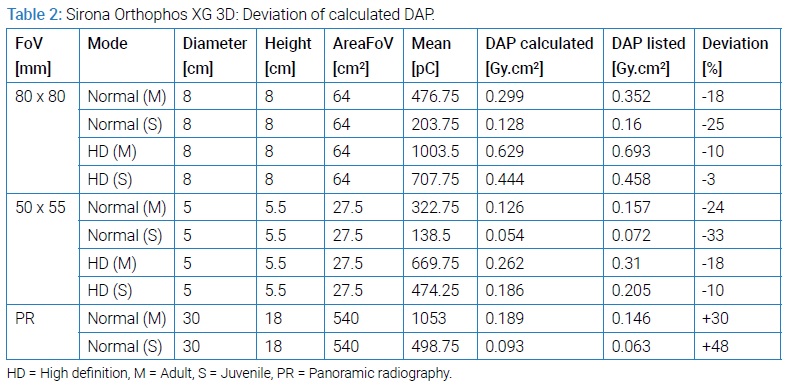
Using several from the manufacturer predefined exposure settings, the radiation doses produced by the two devices Planmeca Promax 3D Max (Planmeca OY, Finland) and Sirona Orthophos XG 3D (Dentsplysirona, Germany) in several 2D and 3D modes were evaluated at the Department of Oral Surgery and Orthodontics, The Medical University of Graz. Therefore, a DAP chamber (Vacu DAP standard; VacuTec GmbH, Dresden, Germany) was positioned at the head of the X-ray tube unit at both devices. As a result of this, a reproducible position was applied. Recordings were performed with several factories pre-sets for each mode. The parameters voxel size (in µm), dimensions of the field of view (FoV in mm), tube voltage (kV), tube current (mA) – which strongly depends on the applied mode and decreases significantly at the juvenile setting –, exposure time (s) and displayed dose area product (DAP in mGy.cm2) were documented. Applied modes for adult and juvenile sizes were “M” and “XS” (Planmeca Promax 3D Max) and “M” and “S” (Sirona Orthophos XG 3D) (Table 1, 2). These were tested in all available accuracy modes: “Normal,” “High Definition” (HD), “High Resolution” (HiRes), “Endo”, “Low Dose” (LD), and “Ultra Low Dose” (ULD) for the Planmeca and “Normal” and “High Definition” (HD) for the Sirona device. To assure reproducibility, measurements were done twice for all modes of the Sirona machine and the smallest FoV of the Planmeca device. All the other measurements for the Planmeca device were checked at random a second time.
The DAP for each recording mode was measured with the DAP chamber. The effective doses for both CBCT devices were then calculated, using the measured DAP, at the Competence Center of Medical Physics and Radiation Protection of the University Hospital, Graz, based on the ICRP 103 directive, using a Monte-Carlo Simulation program (PCXMC, Stuk, Finland) [5]. Therefore, the following parameters were used: measured DAP (mGy.cm2), patient age (30 years for an adult, 15 years for juvenile), tube voltage (kV), filtering (2.5 mm Al / 0.5 mm Cu at Planmeca Promax 3D Max and 2.5 mm Al / 0.3 mm Cu at Sirona Orthophos XG 3D; HVL: > 2.5 mm AI / 90 IEC 60522; -0.3 mm Cu at VOL1/2 at Normal and HD mode), as well as the height and width of the respective FoV. In addition, using coordinates (Xref, Yref, Zref), a point on the virtual phantom was indicated through which the central beam of the CBCT was moved. The projections, the program was contemplating, were made every 10°. A total of 36 projections at a rotation of 360° around the object resulted. The effective dose was finally calculated for each recording mode by synchronizing the established data with the simulation program. To determine the effective dose for the panoramic radiographs, DAP was calculated; the relevant tube current conversion factors from Looe et al. [6] were used. As a result, minimum, maximum, and mean values were calculated depending on the conversion factor applied.
Results
The main results were as follows: There is a wide minimum to a maximum range of effective doses of both investigated X-ray devices from 6 µSv to 16 µSv in 2D modes and 3 µSv to 650 µSv in 3D, which is essentially comparable to previous publications [2]. Second, there is a considerable variation of calculated DAPs compared to DAPs specified by the manufacturer between -3.4% to +55% (mean 26.2%) and -18% to +61% (mean 3.8%) for panoramic radiography and CBCT.
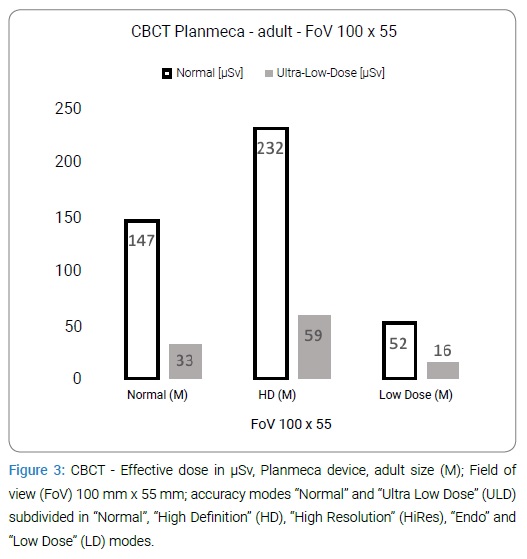
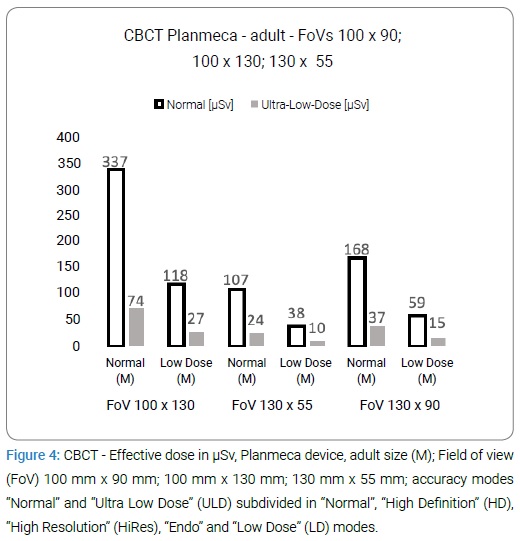
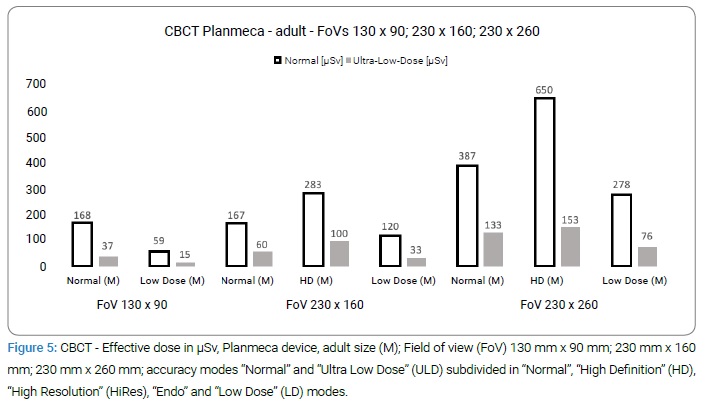
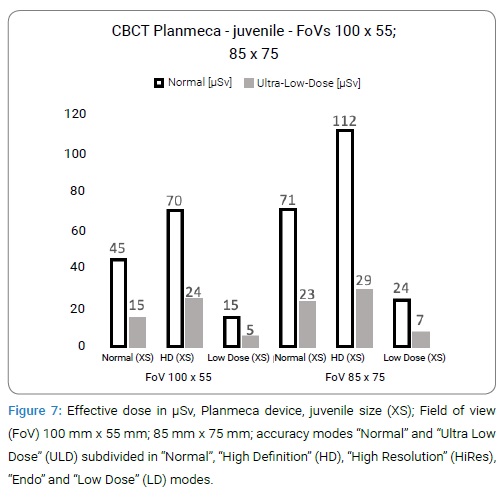
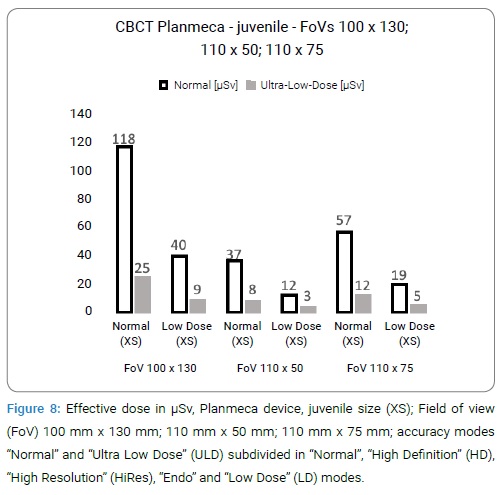
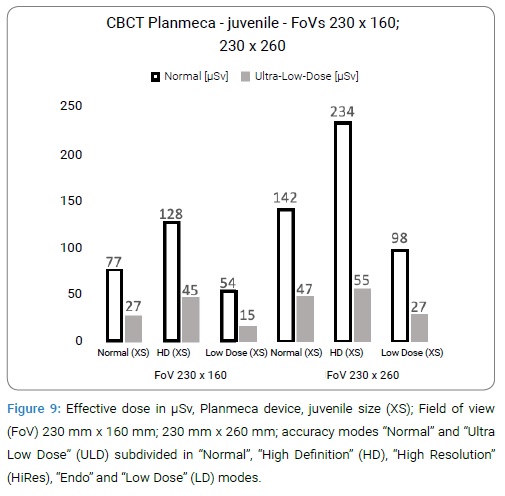
The resulting effective doses strongly depend on the chosen FoV, but also patient size (adult versus juvenile) and particularly on the different resolution modes and can be read off from figures 1−11 [1,4,7]. Planmeca’s ULD mode resulted in a dose of at least 65% and a maximum of 81% lower (mean 74%) in comparison to the other available modes.
The calculated DAPs varied from the DAP displayed on the devices’ control screens. The amount of these variations depended on the device, the FoVs, and the applied modes (2D and 3D, adult and juvenile). For panoramic radiography, DAP calculation showed the highest deviations with the Sirona device, indicating an about 48.4% and 55% higher value compared to listed DAPs. With the Planmeca device, in contrast, deviations were -3.4% and +4.9%.
Referring to 3D, DAP calculations showed the largest discrepancies at the Sirona device (41% to 61% higher compared to listed DAPs; mean 49.9%) with all 3D modes. The lowest deviation was seen at the smallest 50 mm x 55 mm FOV at the Planmeca device (-4% to +5% higher compared to listed DAPs; mean 2.2%). All other FOVs at the Planmeca device showed similar small mean discrepancies ranging from -9.8% to +7.5% lower or higher compared to listed DAPs with an overall range from -18% to +11%.
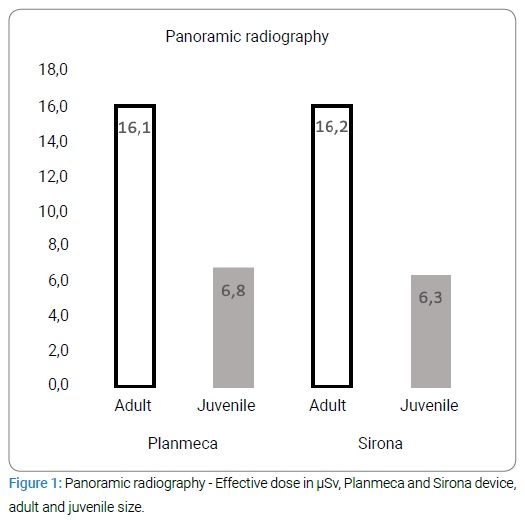
Referring to panoramic radiography, effective doses ranged from 12 μSv to18 μSv and 5 μSv to 7 μSv (adult and juvenile setting) and 17 μSv to 24 μSv in the adult and 7 μSv to 10 μSv in the juvenile mode for Planmeca’s and Sirona’s device (Figure 1).
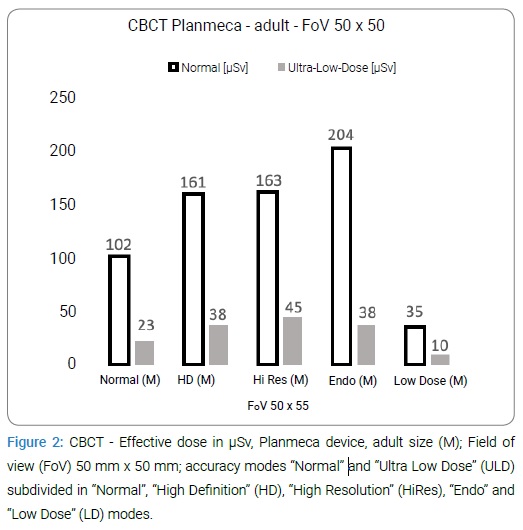
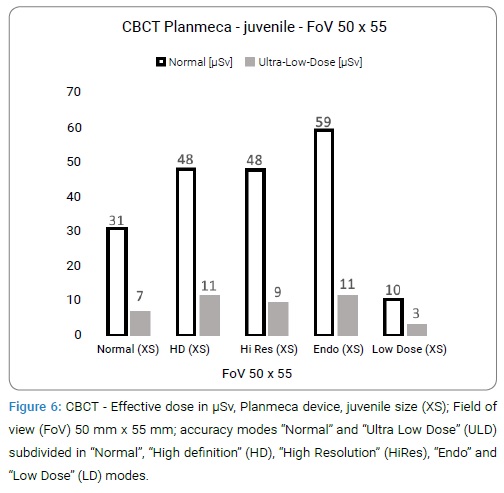
Calculated effective doses for CBCT depended on the chosen FoV. Regarding modes “Normal,” “HD,” “HiRes,” “Endo” and “LD” for the Planmeca device in the adult mode, results varied from 35 μSv to 650 μSv. Additional choosing the ULD mode for all available settings, effective doses decreased and ranged from 10 μSv to 153 μSv. Applying the juvenile setting the modes Normal, HD, HiRes, Endo, and LD with the Planmeca device resulted in doses between 10 μSv to 234 μSv.
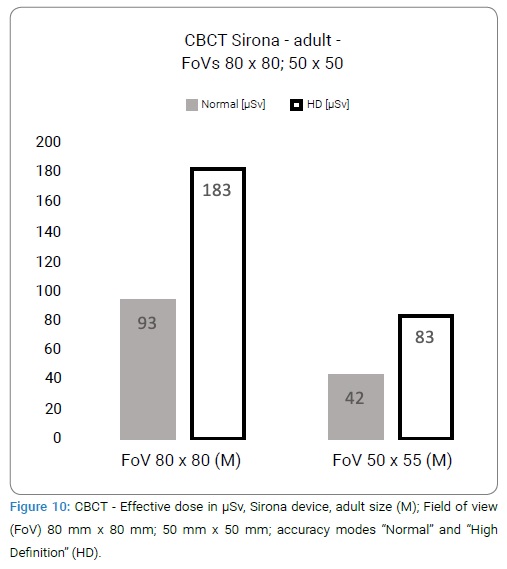
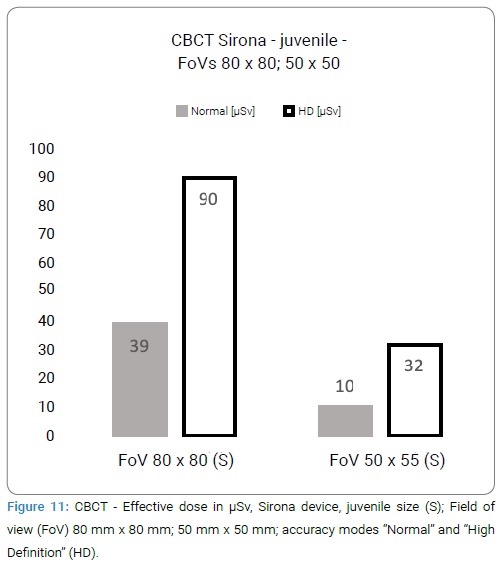
Additional application of the ULD option in the considered modes Normal, HD, HiRes, Endo, and LD with the Planmeca resulted in decreased doses varying between 3 μSv to 55 μSv. For the Sirona device 3D, effective doses ranged from 93 μSv to 183 μSv at the 80 mm x 80 mm FoV and from 42 μSv to 83 μSv at the 50 mm x 50 mm FoV in the adult mode. In juvenile settings, effective doses decreased to 39 μSv to 90 μSv at the 80 mm x 80 mm FoV and 10 μSv to 32 μSv at the 50 mm x 50 mm FoV (Figure 2–11).
Discussion
The two investigated CBCT devices differ in various characteristics, including available FoVs, resolution modes, and the availability of a ULD mode. Concerning the smallest FoVs with comparable size in both investigated devices, the calculated effective doses of the Sirona device, including voxel sizes of 100 μm and 160 μm, range from 42 μSv to 83 μSv for the adult and from 10 μSv to 32 μSv for the juvenile mode. Planmeca’s values, including voxel sizes of 75 μm, 100 μm, 150 μm, and 200 μm, range from 10 μSv to 204 μSv for the adult and 3 μSv to 59 μSv for the juvenile mode. Planmeca’s 75 μm “Endo” mode produces relatively high doses of 204 μSv (adult) and 59 μSv (juvenile), but the ULD mode results in doses around 5 times lower. The 50 mm x 50 mm and 80 mm x 80 mm FoVs of the Sirona device is suggested in the literature as the CBCT volumes for dental use [8–10]. On the other hand, the multiple volume options up to a full skull mode of 230 mm x 260 mm (400 μm; Low Dose and Low Dose-ULD 600 μm) of the Planmeca device are adaptable for more indications, such as orthodontics and maxillofacial surgery. These two devices are typical representatives of the current expanding market [1]. The Sirona device seems to be the more straightforward option for the dentist with a total of 8 different settings, whereas the Planmeca device offers 92 different options. Calculated doses, which range from 3 μSv up to a more than a 200-fold value, confirm that CBCT is not always a dose-saving imaging option [3,4]. However, the use of the ULD mode, which is recommended in the literature Reduces dose values remarkably [11−13]. These low values for the dose-saving ULD modes in this study approach the doses calculated with the panoramic radiography mode. Based on this finding, it seems to be justified to discuss promoting those dose-reduced protocols to replace panoramic radiography as a basic diagnostic tool. However, limitations of the CBCT technique, like requirements for necessary time investment and advanced training as well as possible artifacts, have to be observed. In this context, it has to be considered that the recommended reduction of dose [11] also influences image quality due to modified tube current, tube voltage, and voxel size, even though this was not evaluated here. More options for adjusting the recording parameters might allow more advanced individual decision making and a significant reduction in applied doses, but also demand superior knowledge and skills of the operator, which calls for profound instruction and training for users [12]. Accordingly, the ALARA principle must always be considered and applied [1,14].
As already addressed by Ludlow or Pauwels [2,15], a comparison of dose results between different studies should be done carefully. Even though many studies concerning the evaluation of radiation doses of CBCT devices are available, they often vary in details of methodology or applied settings [2,15]. Further, results can also be influenced by varying device parameters, even of the same brand and type [5]. In former studies dose calculations were often based on traditional TLD measurements [2,15]. While recent studies [11,16–19] have modified their methods toward DAP calculations and Monte Carlo simulations, as performed here. As a consequence, doses agreeing and disagreeing with those documented in this study can be found in the literature [13,16–18]. Shin et al. [13] who used an Alphard 3030 (Asahi Roentgen Ind., Co. Ltd, Kyoto, Japan) device and a calculation of the DAP, yielded for the smallest 51 mm x 51 mm FOV and 100 μm voxel size 81.46 μSv and 428.3 μSv for the largest FoV (200 mm x 200 mm/ 390 μm). Our calculations resulted in 102 μSv (200 μm voxel size) for the smallest FoV and 167 μSv (both Normal mode) for the second-largest FoV (230 mm x 160 mm/ 400 μm). Feragalli et al. [17] recently published juvenile values with 36.8 μSv for a 240 mm x 190 mm FoV (300 μm voxel size) low dose mode. Our calculations resulted in 27 μSv (Normal-ULD 400 μm) and 15 μSv (LD-ULD 600 μm) at the 230 mm x 160 mm FoV. On the other hand, recorded doses published by EzEldeen et al. [18] surpassed the results of this study by far. Results reported by Kim et al. [19] for the 102 mm x 102 mm FoV at the Alphard VEGA device (Asahi Roentgen Ind., Co. Ltd, Kyoto, Japan) are lying at 158 μSv and Koivisto [13]. Showed a dose of 136 μSv at a Promax 3D device with FoV 80 mm x 80 mm. As to calculated panoramic radiography, the mean doses of 6 μSv to 16 μSv reported here tend to correlate with the 2 μSv to 26 μSv of earlier reports. Lee et al. [16,17,20] for instance reported about a range of 8.9 μSv to 37.8 μSv for four different digital panoramic units using an anthropomorphic phantom.
Concerning the used dose calculation method pros and cons have to be discussed. Unlike earlier studies [15], a DAP chamber and a calculation based on the DAP with the Monte Carlo simulation program (PCXMC) were used in this study [5]. Varying deviations in calculated DAPs compared to the displayed DAPs can be seen, but values seem to lie within a limited and acceptable range [13,19]. The greater variance in the Sirona device seems negligible, as these modes produced an acceptable dose outcome compared to the other investigated device. DAP variations up to 70% have also already been reported, which strongly calls for more accurate verifications by medical physicists [17]. The major reason for the use of PCXMC was the simplicity of handling, as has been reported elsewhere [11,13,16,18,19,21] in contrast to the time-consuming use of traditional phantoms [5]. Established in 1997, PCXMC offers the calculation of organ doses for patients of different ages and sizes with adjustable X-ray projections. Age and sex-dependent risk factors can also be included using tissue weighting factors (ICRP 2007) [5]. PCXMC affects the calculation of effective doses, which is relevant when comparing different radiological procedures, even in different hospitals and countries. However, it is not suitable for individual risk assessment, because the risk is also influenced by each patient’s health status and individual sensitivity [5]. Sufficient agreements of calculated results could be shown in different investigations, such as dose measurements and calculations with other phantom models [22–24]. Other literature findings on the use of this technique, however, vary. Ludlow and Ivanovic [25] for instance, calculated about 38% to 62% lower dose values using a single ionization chamber compared to several measurements with an Alderson-Rando phantom, while Kim et al. [19] published 16% to 18% lower doses. In contrast, it has to be mentioned that Zang et al. [21] also reported deviations from different Alderson-Rando phantom evaluations of up to 70%, while SEDENTEXCT guidelines strongly recommend this alternative method to Monte Carlo simulation [12]. Concerning uncertainties of this method, it has to be mentioned that PCXMC depends on X-ray tube output, which varies from device to device due to different physical properties, such as X-ray tube voltage waveform, anode angle, anode surface, filter material in the beam path and incorrectly displayed tube voltage and tube current-time product [5]. Compared to TLD, PCXMC calculations are usually easier to perform [26], however simulation time, ranging from seconds to minutes, depends on the desired accuracy and the speed of the PC. Although, having MC calculations once, doses for many other X-ray spectra can be calculated with little effort [5]. When using PCXMC for panoramic radiography dose calculations this method is not widely accepted. The reason, therefore, is the complex geometry of this kind of diagnostic feature. The rotation center changes continuously and there are uncertainties about the size and passage of the X-ray beam. Lee et al. [26] could show that minor changes in stimulation parameters (e.g. Xref, Yref, Zref, beam height, width, and number of projections) can result in dose variations due to the shift in beam coverage area and affected organs. Further, PCXMC resulted in 9.55% to 51.24% higher dose values compared to TLD measurements. Kim et al. [26,19] also confirmed large dose differences in CBCT measurements when changing the position of the Y and Z axis.
Considering the wide range of dose results within every single device in this study, the ability to handle advanced X-ray devices with sufficient expertise and responsibility seems to be the most important issue regarding their use, especially with children and adolescents [11,27]. Mandatory training which has not been implemented throughout Europe, maybe justified for personnel operating these devices [12].
Conclusion
The results of this study show a wide range of effective doses, strongly depending on the 2D or 3D imaging mode chosen, as well as on the chosen parameters such as FoV, resolution mode, and patient size. Finally, based on the wide range of those dose results, the authors of this study underline the necessity of advanced training for personnel using X-ray devices in dentistry, especially when 3D modes are applied.
References
- Jacobs R, Salmon B, Codari M, Hassan B, Bornstein MM. Cone-beam computed tomography in implant dentistry: recommendations for clinical use. BMC Oral Health. 2018;18(1):88.
- Ludlow JB, Timothy R, Walker C, Hunter R, Benavides E, Samuelson DB, et al. Effective dose of dental CBCT-a meta-analysis of published data and additional data for nine CBCT units. Dentomaxillofac Radiol. 2015;44(1):20140197.
- Widmann G, Al-Ekrish AA. Ultralow Dose MSCT Imaging in Dental Implantology. Open Dent J. 2018;12:87–93.
- Bornstein MM, Brugger OE, Janner SF, Kuchler U, Chappuis V, Jacobs R, et al. Indications and Frequency for the Use of Cone Beam Computed Tomography for Implant Treatment Planning in a Specialty Clinic. Int J Oral Maxillofac Implants. 2015;30(5):1076–1083.
- Tapiovaara M, Siiskonen T. PCXMC - A Monte Carlo program for calculating patient doses in medical X-ray examinations. 2008.
- Looe HK, Eenboom F, Chofor N, Pfaffenberger A, Steinhoff M, Ruhmann A, et al. Conversion coefficients for the estimation of effective doses in intraoral and panoramic dental radiology from dose-area-product values. Radiat Prot Dosimetry. 2008;131:365–373.
- Jacobs R. Dental cone-beam CT and its justified use in oral health care. JBR-BTR. 2011;94(5):254–265.
- Horner K, O’Malley L, Taylor K, Glenny A-M. Guidelines for clinical use of CBCT: A review. Dentomaxillofac Radiol. 2015;44(1):20140225.
- Harris D, Horner K, Grondahl K, Jacobs R, Helmrot E, Benic GI, et al. E.A.O. guidelines for the use of diagnostic imaging in implant dentistry 2011. A consensus workshop organized by the European Association for Osseointegration at the Medical University of Warsaw. Clin Oral Implants Res. 2012;23(11):1243–1253.
- Horner K, Islam M, Flygare L, Tsiklakis K, Whaites E. Basic principles for use of dental cone beam computed tomography: consensus guidelines of the European Academy of Dental and Maxillofacial Radiology. Dentomaxillofac Radiol. 2009;38(4):187–195.
- Marcu M, Hedesiu M, Salmon B, Pauwels R, Stratis A, Oenning ACC, et al. Estimation of the radiation dose for pediatric CBCT indications: a prospective study on ProMax3D. Int J Paediatr Dent. 2018;28(3):300–309.
- SEDENTEXCT. 2018; Accessed 05/18, 2019.
- Koivisto J, Kiljunen T, Tapiovaara M, Wolff J, Kortesniemi M. Assessment of radiation exposure in dental cone-beam computerized tomography with the use of metal-oxide semiconductor field-effect transistor (MOSFET) dosimeters and Monte Carlo simulations. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114(3):393–400.
- Oenning AC, Jacobs R, Pauwels R, Stratis A, Hedesiu M, Salmon B, et al. Cone-beam CT in pediatric dentistry: DIMITRA project position statement. Pediatr Radiol. 2018;48(3):308–316.
- Pauwels R, Beinsberger J, Collaert B, Theodorakou C, Rogers J, Walker A, et al. Effective dose range for dental cone beam computed tomography scanners. Eur J Radiol. 2012;81(2):267–271.
- Shin HS, Nam KC, Park H, Choi HU, Kim HY, Park CS, et al. Effective doses from panoramic radiography and CBCT (cone beam CT) using dose area product (DAP) in dentistry. Dentomaxillofac Radiol. 2014;43(5):20130439.
- Feragalli B, Rampado O, Abate C, Macri M, Festa F, Stromei F, et al. Cone-beam computed tomography for dental and maxillofacial imaging: technique improvement and low-dose protocols. Radiol Med. 2017;122(8):581–588.
- EzEldeen M, Stratis A, Coucke W, Codari M, Politis C, Jacobs R, et al. As Low Dose as Sufficient Quality: Optimization of Cone-beam Computed Tomographic Scanning Protocol for Tooth Autotransplantation Planning and Follow-up in Children. J Endod. 2017;43(2):210–217.
- Kim EK, Han WJ, Choi JW, Battulga B. Estimation of the effective dose of dental cone-beam computed tomography using personal computer-based Monte Carlo software. Imaging Sci Dent. 2018;48(1):21–30.
- Lee GS, Kim JS, Seo YS, Kim JD. Effective dose from direct and indirect digital panoramic units. Imaging Sci Dent. 2013;43(2):77–84.
- Zhang G, Marshall N, Bogaerts R, Jacobs R, Bosmans H. Monte Carlo modeling for dose assessment in cone-beam CT for oral and maxillofacial applications. Med Phys. 2013;40(7):072103.
- Schmidt PW, Dance DR, Skinner CL, Smith IA, McNeill JG. Conversion factors for the estimation of effective dose in pediatric cardiac angiography. Phys Med Biol. 2000;45(10):3095–3107.
- Schultz FW, Geleijns J, Spoelstra FM, Zoetelief J. Monte Carlo calculations for assessment of radiation dose to patients with congenital heart defects and to staff during cardiac catheterizations. Br J Radiol. 2003;76(909):638–647.
- Helmrot E, Pettersson H, Sandborg M, Altén JN. Estimation of dose to the unborn child at diagnostic X-ray examinations based on data registered in RIS/PACS. Eur Radiol. 2007;17(1):205–209.
- Ludlow JB, Ivanovic M. Comparative dosimetry of dental CBCT devices and 64-slice CT for oral and maxillofacial radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106(1):106–114.
- Lee C, Lee S-S, Kim J-E, Huh K-H, Yi W-J, Heo M-S, et al. Comparison of dosimetry methods for panoramic radiography: thermoluminescent dosimeter measurement versus personal computer-based Monte Carlo method calculation. Oral Surgery, Oral Surg Oral Med Oral Pathol Oral Radiol. Invalid date. 2016;121(3):322–329.
- Pauwels R, Zhang G, Theodorakou C, Walker A, Bosmans H, Jacobs R, et al. Effective radiation dose and eye lens dose in dental cone beam CT: effect of field of view and angle of rotation. Br J Radiol. 2014;87(1042):20130654.
Keywords
Monte carlo simulation; Effective dose; CBCT; Panoramic radiography
Cite this article
Kirnbauer B, Rugani P, Guss H, Stücklschweiger G, Jakse N. Effective dose of two CBCT and panoramic radiography hybrid devices using a DAP-based method. Clin Surg J. 2021;2(3):1–9.
Copyright
© 2021 Kirnbauer Barbara. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
